




TL;DR:
- Most small practices are working on the billing process, submitting claims, posting payments, chasing denials, and still leaving money on the table.
- The problem isn’t effort. It’s that no one owns each stage end-to-end, so errors pass through quietly and compound.
- Revenue cycle management works when every stage has a clear owner tracking their own metrics, not just completing tasks.
- Practices that fix the structure collect more—using healthcare virtual assistant services like Wing to bring ownership to each stage
Most small practices aren’t losing revenue because of bad care or bad staff; they’re losing it because their billing process has gaps nobody officially owns.
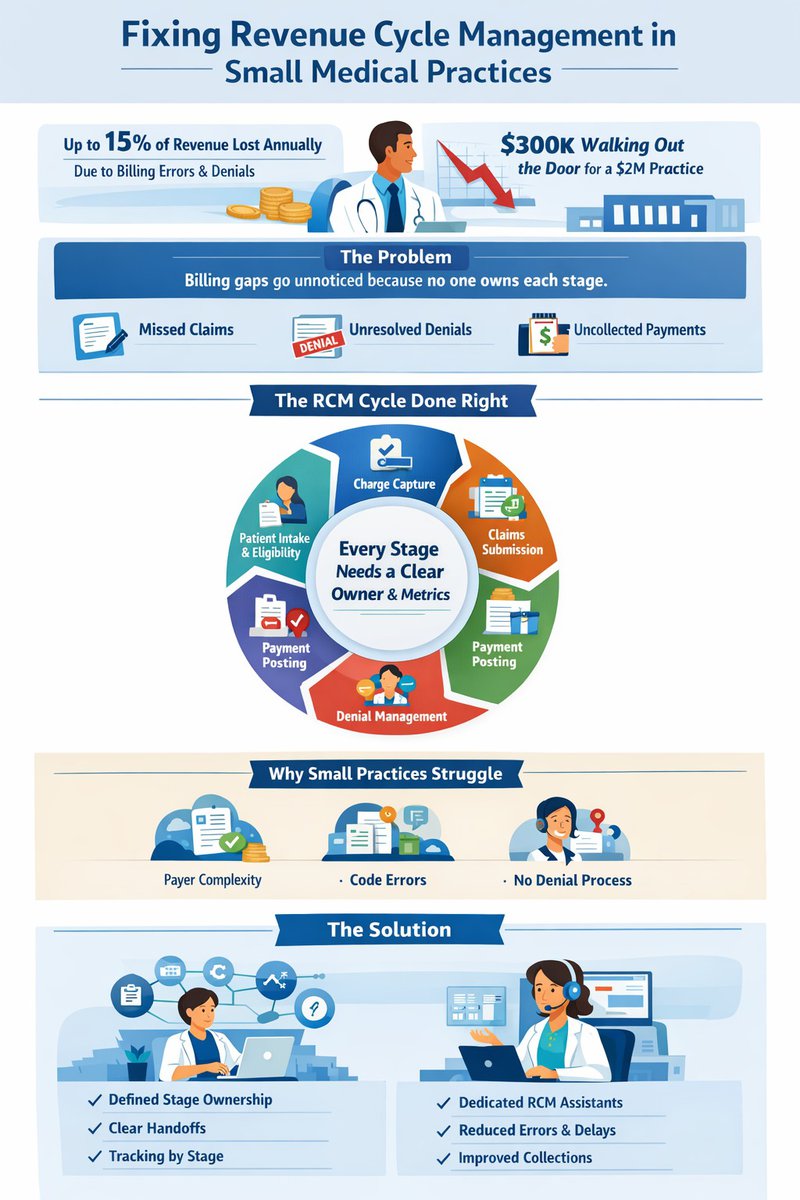
According to the Medical Group Management Association (MGMA), physician practices lose up to 15% of revenue annually due to billing errors, claim denials, and poor follow-up. For a practice doing $2M a year, that’s $300,000 quietly walking out the door.
In this article, we break down what revenue cycle management actually looks like for small practices, where the real breakdowns happen, and what a more structured approach does to fix it.
The Billing Problem Isn’t What You Think It Is
Small medical practices consistently collect less than they’re owed. Not because the work wasn’t done or the claims weren’t submitted, but because revenue leaks at multiple handoff points between patient intake and final payment. A denial comes back. Someone handles it when they can. A follow-up falls through. The write-off gets logged, and the cycle repeats.
The common read on this: the team is stretched too thin. More staff, or better-trained staff, would solve it. That explanation feels reasonable, and it’s mostly wrong.
The actual problem is structural. Revenue cycle management in small practices is typically distributed across two or three people who each handle several roles. When a step fails, there’s no clear owner for the recovery. The error doesn’t get caught; it gets absorbed, quietly, into the next billing period.
What Revenue Cycle Management Actually Covers
Revenue cycle management (RCM) is the end-to-end process of capturing and collecting payment for clinical services. It begins before the patient walks in and ends when the account is fully reconciled.
The cycle has six core stages:
- Patient registration and eligibility verification — Accurate demographic and insurance data captured at scheduling or intake. Eligibility verified before the appointment. Errors here cascade through every stage that follows.
- Charge capture — Clinical services translated into billable codes. Missed or inaccurate codes directly reduce collectible revenue. This is where underbilling most often originates.
- Claims submission — Clean claims submitted to the correct payer within filing deadlines. A clean claim has accurate codes, correct patient data, and proper modifiers. Anything else triggers a rejection or denial.
- Payment posting — Payments from payers and patients are matched to the correct account. Posting errors creates false balances, complicates follow-up, and slows down the entire cycle.
- Denial management — Denied claims reviewed, corrected, and resubmitted within appeal windows. This stage is where most small practices lose money—not through single large failures, but through small denials left unworked.
- Patient collections — Remaining patient balances are billed, tracked, and collected. With high-deductible plans increasingly common, this stage carries more revenue weight than it did five years ago.
Each stage depends on the accuracy of the stage before it. That dependency is the structural reality most small practices don’t fully account for.
Why Small Practices Struggle with RCM
Large systems have entire departments dedicated to each RCM stage. Most small practices run the same cycle with two or three people who also handle phones, referrals, and authorizations. When something urgent lands, the denial queue waits. The follow-up doesn’t happen.
Three factors make it harder:
- Payer complexity. Every commercial payer has its own rules, filing limits, and appeal procedures. Without documented workflows, that knowledge lives in someone’s head and walks out when they leave.
- Code accuracy. One wrong modifier on a high-frequency service can quietly cut reimbursement by 20–40% across hundreds of claims before anyone spots the pattern.
- No real denial process. Most practices check the denial queue “when there’s time.” That’s not a workflow. It’s how revenue disappears without anyone noticing.
The Fix: Build Ownership Into the Cycle
The dominant RCM approach in small practices is task-based. Staff work a list each day to submit claims, post payments, and check denials. When the list is completed, it resets. But patterns don’t get noticed, and the same errors repeat.
The more durable model is stage ownership. Each stage has a defined owner responsible not just for completing the task, but for the accuracy of what comes in and the quality of what goes out. Stage owners track their own metrics, such as denial rates by payer, days in A/R, and clean claim rate to catch problems before they compound.
This doesn’t require more staff. It requires clarity:
- Define who owns each stage — not just who works it, but who is accountable for its output.
- Set handoff standards — so errors don’t silently pass from one stage to the next.
- Track by stage, not just totals — a global collections number hides where the cycle is actually breaking.
The difference between task completion and stage ownership is the difference between “I submitted the claims” and “I submitted 98 clean claims, and the 2 rejections are in active follow-up.” One tells you work happened. The other tells you the cycle is healthy.
For practices that don’t have the internal bandwidth to build this structure, Wing Assistant offers dedicated remote billing support. Wing’s virtual assistants are trained staff who work as an extension of your team, with defined responsibilities across the RCM cycle. It’s a practical way to add accountability and follow-through without the overhead of a full in-house hire.
In-House or Outsourced: What Works and When
Before deciding anything, most small practices have real improvement available within their current setup. A few moves that consistently make a difference:
- Standardize the front end. Verify eligibility and confirm demographics before every appointment. Errors caught here don’t become denials later.
- Set a denial response window. Denials worked within 7 days recovered at significantly higher rates than those treated at 30+. Even a dedicated two-hour block weekly creates structure where there currently isn’t any.
- Document payer-specific rules. For the 5–8 payers driving 80% of your volume, write down their filing limits, common denial reasons, and appeal steps. Stop relying on institutional memory.
- Break down your A/R by age. A single days-in-A/R number hides where revenue is actually sitting. Segment it: 0–30, 31–60, 61–90, 90+. The 90+ bucket is where money goes to disappear.
Once the process is defined in-house, the question becomes whether to keep it there or hand it off. Here’s how the two paths compare:
| In-House | Outsourced | |
|---|---|---|
| Cost | Lower upfront, but staff time is real cost | Predictable monthly fee, often % of collections |
| Control | Full visibility and direct management | Depends on vendor reporting and communication |
| Expertise | Limited to what your team knows | Access to payer specialists and dedicated denial staff |
| Scalability | Harder to scale without hiring | Scales with volume without headcount changes |
| Risk | Staff turnover disrupts the cycle | Vendor performance risk; less institutional knowledge |
| Best for | Practices with stable volume and a defined process | Practices with denial rates above 10% or A/R over 90 days exceeding 15% |
Outsourcing doesn’t remove the need for oversight, but it shifts it. Instead of managing a billing team, you’re reviewing performance metrics and managing a vendor relationship. The accountability structure still matters either way.
Why Small Practices Choose Wing for RCM Support
Most outsourced billing solutions hand you a system. Wing gives you a dedicated, HIPAA-trained healthcare virtual assistant who owns their stage of the cycle and shows up every day.
The results from medical practices speak for themselves:
- 50% faster clinic admin workflows
- 35% reduction in billing errors
- 25% fewer scheduling errors and 25% faster claims processing
- 40% higher patient satisfaction scores
- 25+ hours per week saved on clinic admin
- 50% fewer emails and manual follow-ups handled by the clinical team
At Provida Family Medicine, Wing’s healthcare VAs took over EHR updates, patient intake, and insurer coordination, cutting errors and clearing the internal team to focus on patient care.
The difference with Wing isn’t just the cost savings; it’s that the assistant is accountable, managed, and built into your workflow from day one. No lengthy hiring process. No training from scratch. No coverage gaps when someone leaves.
FAQs
1. What actually changes when you add a healthcare virtual assistant to billing?
The work stops between steps. Claims get followed up, denials get resubmitted, and A/R gets worked consistently. Your virtual assistant handles the day-to-day execution inside your systems, while you stay in control of how the process runs.
2. Do I lose visibility or control if I use a virtual assistant for billing?
No. Your virtual assistant works inside your EHR and billing tools, following your workflows. You decide priorities, review outcomes, and stay as hands-on as you want. The difference is you’re no longer chasing tasks to keep things moving.
3. When does it make sense to use virtual assistant services for RCM?
When the work is getting done inconsistently, not incorrectly. Most small practices don’t need more strategy; they need consistent follow-through. A dedicated healthcare virtual assistant fills that gap without the cost or risk of hiring in-house.
Stop Losing Revenue to a Broken Process
The practices that consistently collect what they earn don’t have bigger billing departments. They have clearer cycles. Every stage has an owner. Every handoff has a standard. Performance is tracked by stage, not by global metrics that obscure where the friction actually lives.
If your collections aren’t reflecting your clinical volume, the gap isn’t effort. It’s structure, and that’s exactly what Wing is built to fix.
Book a free demo with Wing today and see how a dedicated healthcare virtual assistant can close the gaps in your revenue cycle.

Dianne Florendo is a content writer who creates engaging SEO content about virtual assistants, outsourcing, and business productivity.



