





TL;DR
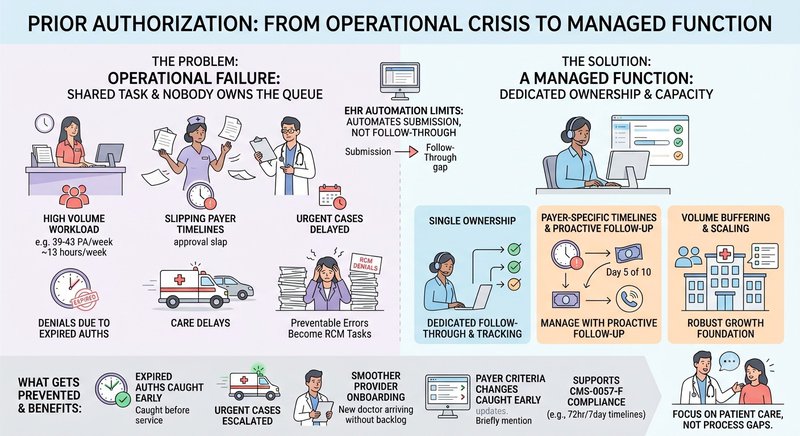
Prior authorization is most often discussed as a physician burnout issue, but the operational problem is a capacity and ownership one: someone has to own the queue, track payer timelines, and follow up before care is delayed. With an average of 39–43 prior authorizations per physician per week and payer rules changing constantly, practices that treat prior authorization services as a shared task rather than a dedicated function end up with denied claims, delayed care, and the administrator absorbing the follow-up.
The Numbers Are Not a Burnout Story: They're a Workload Story
The AMA's 2024 prior authorization survey puts the volume at 39–43 prior authorizations per physician per week. Each one requires a submission, a payer timeline to track, and in many cases a follow-up call or peer-to-peer review before it resolves. Across a practice, that adds up to roughly 13 hours of clinical and administrative staff time per physician per week, time spent on a process that produces no clinical output.
Ninety-four percent of physicians link prior authorization directly to burnout. That stat gets cited constantly in policy debates about reform, and it should. But for the practice administrator, it points to a different problem: all that follow-up time is landing somewhere. When physicians are spending their evenings on peer-to-peer calls and their nurses are fielding payer callbacks between patient visits, the prior auth queue isn't being managed; it's being absorbed by whoever happens to be available.
That's a capacity and ownership problem, not a clinical one. And it's one that operations can actually solve.
The Real Issue: Nobody Owns the Queue
In most practices, prior authorization is handled by whoever has time. A front-desk coordinator submits the initial request. A nurse follows up when a patient calls asking why their approval hasn't come through. A physician takes the peer-to-peer call when a denial lands. The biller flags it during claim review when the auth was expired by the time the service was rendered.
Everyone touches it. Nobody owns it.
This creates three compounding failure points:
Payer timelines slip. Prior authorization approvals have expiration windows, often 60 to 90 days. When no one is actively tracking the queue, services get rendered after approval expires. The claim is submitted, the payer denies it for missing or expired auth, and what should have been a preventable error becomes a rework task requiring an appeal.
Urgent cases don't get escalated. Not all prior auths carry the same urgency. A scheduled elective procedure has a margin. A patient waiting for oncology treatment does not. Without a dedicated function managing the queue by priority and payer response time, urgent cases get processed in the same order as everything else, or not at all until a physician calls someone in a panic.
Denials route back to the administrator anyway. The downstream denial lands in the RCM workflow. Someone has to work it, appeal it, or write it off. That cost, in staff time, in delayed reimbursement, in potential write-offs — originated from a prior authorization that wasn't tracked properly. The administrator owns the consequence even when the process was never structured for accountability.
Why EHR Automation Has Not Solved This
The pitch for EHR-integrated prior auth tools is a reasonable one: automate submission, reduce manual work, speed up approvals. Several EHR platforms now include electronic prior auth functionality, and CMS's interoperability and prior authorization rule (CMS-0057-F) is pushing payers to support API-based submissions on an accelerating timeline through 2026–27.
But the tools route the request. They don't follow it through payer timelines.
Electronic submission gets the initial request to the payer faster. It doesn't call the payer when day ten arrives, and there's been no response on a case that's blocking a procedure scheduled for day twelve. It doesn't catch that a payer changed its criteria for a specific CPT code last quarter, and the practice's template is now submitting incomplete clinical documentation. It doesn't prioritize the queue when two urgent cases land on the same day a new provider's credentialing finishes, and their first week of scheduled patients suddenly need active authorizations.
The gap is in the follow-through, and follow-through requires a person with capacity and accountability to do it consistently.
The Scaling Problem Nobody Plans For
Most practices absorb prior auth volume until they can't. Then they hire someone, split responsibilities, or reassign tasks, and repeat the cycle when volume climbs again.
The trigger points that cause the most disruption:
A new provider joins. Their first few weeks of scheduled patients arrive needing authorizations, often across payers the existing staff is less familiar. The queue spikes. Existing staff absorb it until errors start appearing.
A payer updates its criteria. A major commercial payer tightens documentation requirements for a service line that the practice frequently authorizes. Without someone actively monitoring payer policy changes, the practice keeps submitting under the old template. Denial rates rise before anyone connects the cause.
A new payer panel opens. Taking on a new payer relationship means learning a new portal, a new timeline, new criteria, and new escalation contacts. That learning curve lands on whoever currently handles prior authorization services, likely as an addition to their existing workload, not a replacement for it.
None of these is an unusual event. They're the normal operating conditions of a growing practice. But each one adds queue volume without adding capacity to work it, which is why prior auth remains a persistent problem even at practices that have nominally "solved" it before.
What a Managed Prior Auth Function Actually Looks Like
Forty percent of practices now have staff exclusively dedicated to prior authorization services, according to the AMA's 2024 data. That's meaningful, but it leaves sixty percent of practices still running prior authorization as a shared task, and even dedicated in-house staff face the same scaling constraints when volume spikes or a team member turns over.
The functional model that prevents the failure points above has a few consistent characteristics:
Single ownership of the queue
One person or team is accountable for every open authorization, submission status, payer response timeline, escalation trigger, and expiration date. Nothing moves to the next step without that owner's awareness.
Payer-specific timeline tracking
Different payers respond on different timelines. Medicare Advantage plans, commercial insurers, and Medicaid each have their own review windows and escalation paths. A managed function tracks these by payer, not by a generic "follow-up in five days" rule.
Active follow-up before deadlines, not after
The standard failure mode is reactive: someone calls the payer after a denial or an expired auth. A managed function calls before, at day five if the payer's SLA is ten days, at the halfway point of an approval window before a scheduled service.
Volume buffering for practice growth
When a new provider joins or a payer panel expands, the prior authorization services absorbs the volume spike without pulling nurses off the floor or dumping the overflow on the administrator.
Wing's Prior Authorization Specialists work this way, managing the queue inside existing payer portals and EHR systems, tracking payer timelines by insurer, and following up proactively before approvals expire or care gets delayed. Wing assistants are AI-trained, ISO 27001 compliant, and SOC 2 certified, which matters for practices navigating the data-sharing requirements that come with CMS-0057-F's phased rollout through 2026–27.
The same function extends to adjacent RCM tasks: insurance verification services before appointments, insurance eligibility verification services at scheduling, and denial management when prior auth failures create downstream claim rejections, which they consistently do when the queue isn't owned.
The Regulatory Timeline Is Adding Pressure
CMS-0057-F requires covered payers to respond to prior auth requests within 72 hours for urgent cases and seven calendar days for standard requests, with phased implementation running through 2026–27. The rule also mandates that payers provide a specific reason when denying a request and that they support electronic prior auth data exchange through standardized APIs.
This is a tailwind for practices that already have structured prior authorization services; faster payer response times mean faster approvals, and electronic submission makes the workflow more trackable. But it's also new complexity: practices will need to monitor whether their payers are meeting the mandated timelines, document denial reasons for appeal, and adapt to API-based submission requirements across their payer mix.
That's more work for a function that's already under-resourced at most practices. A dedicated Prior Authorization Specialist absorbs that compliance work. A shared-responsibility model pushes it onto whoever is already overwhelmed.
What Gets Prevented When Someone Owns It
The downstream effects of unmanaged prior authorization are well-documented: denied claims, delayed care, administrative rework, and physician burnout from follow-up calls that shouldn't require physician involvement. The less-discussed effect is what gets prevented when the function is owned.
- Expired authorizations caught before the service date, not after the claim is denied
- Urgent cases escalated through payer peer-to-peer before the scheduled procedure
- New provider onboarding absorbed without a queue backlog
- Payer criteria changes caught early through active portal monitoring
- Denial rate held flat while the practice adds providers and expands payer panels
Prior authorization isn't going to get simpler. Payer requirements are tightening, regulatory timelines are compressing, and practice volumes are growing. The practices that treat it as a managed function, with ownership, accountability, and dedicated capacity, are the ones that stop absorbing the downstream cost.
The ones that don't will keep routing it back to the administrator.
See how Wing manages prior auth from submission to approval → Book a Demo

Dianne Florendo is a content writer who creates engaging SEO content about virtual assistants, outsourcing, and business productivity.



