





The real cost of a rising claim denial rate is not the denial itself; it is the appeals capacity required to recover the revenue. Approximately 90% of denied claims are ultimately paid, but only if someone actively works the appeals queue. When A/R sits past 90 days, and the RCM team is already at capacity, the money exists on paper but is not being collected.
The Benchmark Nobody Wants to Own
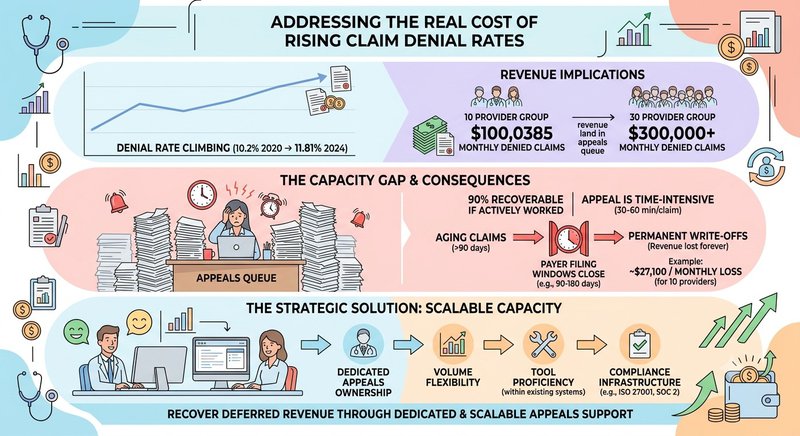
The industry denial rate hit 11.81% in 2024, up from 10.2% in 2020. That four-year climb looks modest on a chart. It is not modest in a billing department.
For a 10-provider group averaging $85,000 in monthly claims per provider, roughly $850,000 in total monthly volume, an 11.81% denial rate means $100,385 in denied claims landing in the appeals queue every month. At a 30-provider group, that number is $300,000. Every month.
The standard response is to tighten the front end: clean up coding, scrub claims before submission, and reduce the denial rate. That is the right long-term play. But it sidesteps the more immediate problem, which is what happens to the $100,000 that is already denied and sitting in the queue right now. For most mid-size groups, that is where medical billing outsourcing enters the conversation, not as a cost-cutting measure, but as the only realistic way to staff the appeals function at the volume it actually requires.
The Money Is There. The Capacity to Recover It Usually Isn't.
Roughly 90% of denied claims are ultimately paid, which means denial revenue is not lost; it is deferred. The recovery depends entirely on whether someone actively works the appeal.
That word "actively" is doing a lot of work. Working a denial means pulling the EOB, identifying the denial reason code, locating the medical record or prior auth documentation, drafting the appeal letter, submitting through the payer portal, logging the follow-up date, and tracking the outcome. For a single complex denial, that process can take 30 to 60 minutes of skilled billing staff time.
Multiply that by a queue of 200–400 denials per month at a 10-provider group, and you are looking at 100–400 hours of work the team has to absorb on top of claim submission, payment posting, patient billing, and everything else in the workflow.
Most billing teams are not staffed for that. They were staffed for the baseline volume when the group was smaller, or when the denial rate was lower, or before the last payer policy change added a new records-request category. The queue does not disappear; it ages.
What "We'll Work It Later" Actually Costs
A/R over 90 days now sits above 35% market-wide. The historical benchmark target is under 20%. That gap is not an accounting abstraction. It represents real revenue that is increasingly difficult to collect.
Here is why the aging matters: most payer contracts have timely filing windows for appeals — typically 90 to 180 days from the date of service or original denial. Once a claim ages past that window, the denial becomes permanent. A payer that would have paid 90% of the original claim at 60 days will pay nothing at 200 days.
The math for a 10-provider group:
- Monthly claims volume: ~$850,000
- Denied claims at 11.81%: ~$100,385
- Recoverable at 90%: ~$90,347
- If 30% of the queue ages past the filing window, ~$27,100 in permanent write-offs per month
- Annualized: ~$325,000
At a 30-provider group, that number triples. And this calculation assumes denial volume holds steady, which it has not been doing.
The Capacity Trap: Why Growing Groups Are Most Exposed
Every new provider added to a group creates claim volume immediately. A new physician seeing 15 patients per day is generating claims from day one. The RCM team does not grow at the same rate.
The result is a structural capacity gap that compounds with each new hire or site addition. The billing team that handled 10 providers adequately is now managing 14 providers with the same headcount. Denial queue management is usually the first thing that slips; it is time-intensive, it requires experienced judgment, and there is no immediate visible consequence when it is deferred by a week.
Billing-role turnover makes this worse. Turnover in billing functions commonly runs 20–40%. When an experienced biller leaves, institutional knowledge about payer behavior, appeal strategies, and queue status walks out with them. Onboarding a replacement takes months to reach proficiency. In the interim, the queue ages.
Payers Know You Can't Appeal Everything
This is not incidental. Medical-necessity denials rose 5% in 2024. Records-request denials rose 5.4%. Both categories require documentation pulls and manual appeal effort, exactly the type of high-friction work that backs up when a team is stretched.
Payers are increasingly using AI-driven medical-necessity review tools specifically calibrated to generate volume denials at a rate practices cannot fully appeal. The calculation is explicit: if a payer denies 10,000 claims knowing that only 6,000 will be appealed, the 4,000 unworked denials are recovered revenue at zero cost to the payer.
Practices with lean RCM teams are subsidizing that math every month. The answer is not just submitting cleaner claims; it is building appeals capacity that scales with denial volume regardless of what payers do next year.
What a Scalable A/R Model Actually Requires
Sustainable denial management is a function, not a task. It requires:
- Dedicated ownership — someone whose primary job is the denials queue, not billing generalist work that includes denials as one of fifteen responsibilities
- Volume flexibility — capacity that increases when a new site comes on or a payer changes policy, rather than a headcount request that takes three months to approve and fill
- Tool proficiency — working inside the practice's existing billing system from day one, not a six-week ramp to learn the platform
- Compliance infrastructure — HIPAA-compliant workflows, documented access controls, and audit-ready processes
For most mid-size groups, the answer is not hiring another full-time biller. It is medical billing outsourcing structured around function-level ownership, dedicated appeals capacity that scales with volume rather than absorbing the backlog onto a team already stretched thin.
When evaluating medical billing outsourcing services, the distinction that matters is whether the model gives you a dedicated resource working your queue or a shared pool that deprioritizes your denials when another client's volume spikes. The same logic applies to healthcare revenue cycle outsourcing broadly; shared-resource models create the same capacity gap you are trying to solve.
A medical billing audit is often the right starting point: identify where denials are clustering, which payer relationships are generating the most friction, and where the A/R aging is concentrated before adding capacity. That audit surfaces whether the fix is upstream (coding, prior auth) or downstream (appeals ownership, A/R follow-up).
How Wing Supports Denial and A/R Management
Wing provides dedicated RCM services, Denials Management Specialists, Medical Billing Specialists, Medical Coding Specialists, and Medical Insurance Verification Specialists, who work inside your existing billing system from day one.
Wing assistants are AI-trained and proficient across modern RCM platforms. As a dedicated healthcare RCM services provider, Wing deploys assistants as single-client resources, not shared support pools, which means the assistant working your denials queue is not also handling unrelated work for other clients. When volume increases because a new provider joins or a payer changes its medical-necessity criteria, capacity scales with it.
Wing is ISO 27001 compliant and SOC 2 certified, with HIPAA-aligned workflows built into every engagement.
For practice administrators evaluating how to outsource medical billing without losing visibility into the A/R, Wing's model keeps your team in the workflow, you retain oversight, and Wing handles the queue volume. The full scope of Wing's revenue cycle management support and healthcare BPO services is available for groups mapping where dedicated RCM ownership fits their current structure.
See how Wing keeps the denial queue from backing up → Book a Demo

Dianne Florendo is a content writer who creates engaging SEO content about virtual assistants, outsourcing, and business productivity.



