




TL;DR
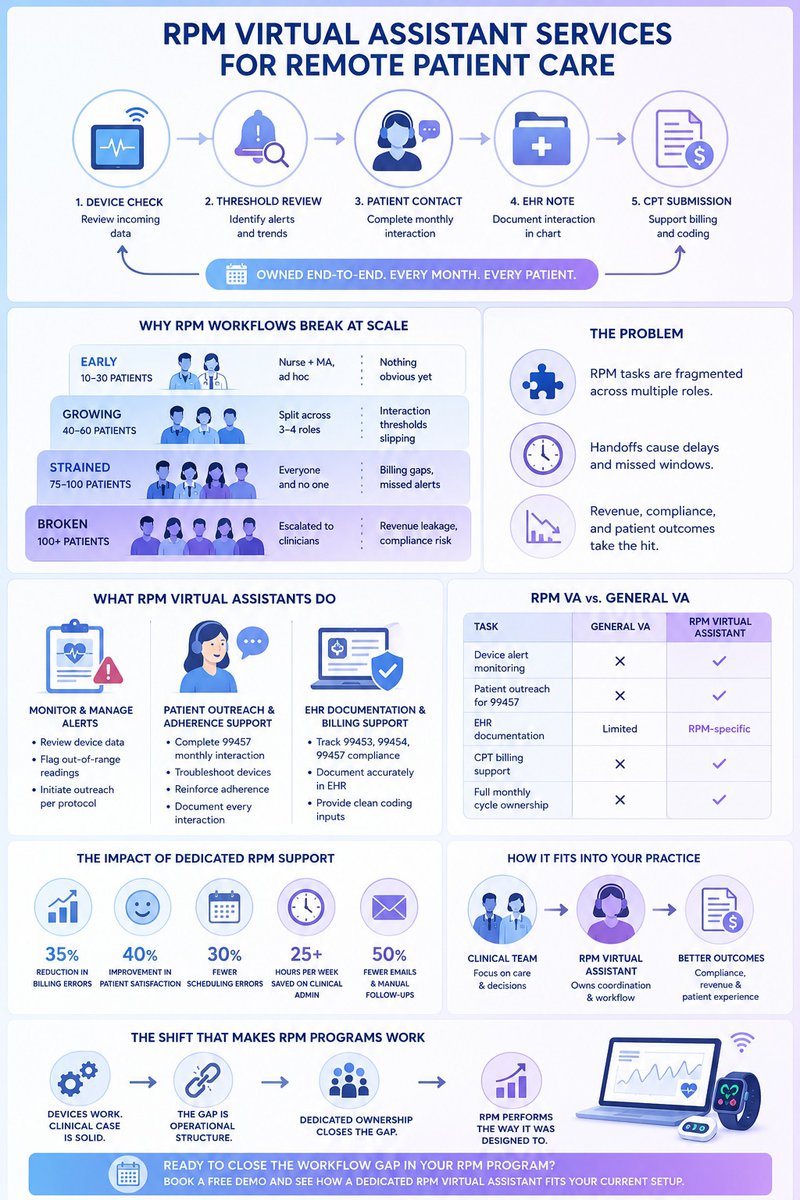
- When RPM volume grows, most practices spread the work across MAs, coordinators, and whoever's available; nobody owns it end-to-end.
- The 20-minute interaction requirements slip. Alerts sit. Billing goes out incomplete. The program underperforms, and nobody's sure why.
- A dedicated RPM virtual assistant owns the full cycle, device review, patient outreach, EHR notes, and billing inputs every month, every patient.
- The program stops leaking and starts performing the way it was projected to.
RPM adoption is accelerating. According to the American Medical Association, RPM use among physicians nearly tripled between 2016 and 2022, yet most practices still haven't solved the operational side of running these programs at scale.
The clinical case for remote patient monitoring is settled. The workflow case is where most programs break down. This guide covers what RPM virtual assistant services actually do, how they differ from general VA support, which tasks they own, and what to look for when choosing a provider.
Wing Assistant specializes in this workflow, built specifically for the coordination, documentation, and billing cycle that RPM programs require to perform the way they were designed to.
When RPM Workload Outpaces Staff Capacity
Remote patient monitoring works on paper — devices collect data, alerts flag anomalies, and clinicians intervene earlier. The clinical logic is sound. The operational logic breaks faster than most practices expect.
Here's what that typically looks like in practice:
- Low enrollment (10–20 patients): The workflow feels manageable. An MA reviews the dashboard, someone returns a patient call, and a note gets added to the chart. It's absorbed into existing roles.
- Growing enrollment (40–60 patients): Alert queues start backing up. Monthly interaction requirements go untracked. Billing closes with incomplete documentation.
- Scaled enrollment (75–100+ patients): The program that was supposed to generate revenue starts creating compliance exposure instead.
The bottleneck isn't effort. It’s structure, no single person owns the RPM loop end to end. RPM virtual assistant services exist to close that gap directly.
Why Assigning RPM to Existing Staff Doesn't Scale
The instinct when RPM volume increases is to distribute the work more clearly — tighter SOPs, specific task assignments, a new checklist. That's reasonable. It's also insufficient.
The core problem: RPM is a continuous loop with time-sensitive triggers at every stage. No generalist role is designed to own it end-to-end.
Here's why it breaks down:
- MAs, coordinators, and front-desk staff already carry full primary responsibilities. RPM tasks get handled in the gaps, which means inconsistently.
- No single person tracks the full cycle device check, threshold review, patient contact, EHR note, and CPT submission, so handoffs create delays, and accountability diffuses.
- Delays in RPM compliance mean missed billing windows, claim denials, and revenue leakage that compounds month over month.
The missing variable isn't a better process document. It's dedicated workflow ownership — a role whose only job is moving RPM patients through the monitoring cycle, on time, every month.
That's the structural difference RPM virtual assistant services provide.
How the Workflow Fragmentation Builds
The fragmentation doesn't start as a crisis. It starts as a reasonable workaround — and stays invisible until volume forces it into view.
Early stage (20–30 patients):
- Device vendor handles setup
- A nurse reviews the dashboard when time permits
- Billing submits based on whatever's in the chart
- It works — loosely
Growth stage (50–60 patients):
- Alert volume increases, but the nurse is also doing in-person triage
- The MA handling outreach is also managing scheduling
- The 99457 interaction threshold goes untracked before billing windows close
What locks it in:
- The program still produces some revenue, so the dysfunction isn't immediately visible
- Leadership sees partial results and assumes the workflow is functioning
- The structural gap compounds quietly until volume makes it undeniable
| RPM Stage | Patient Volume | Who’s Handling It | What’s Breaking |
|---|---|---|---|
| Early | 10–30 | Nurse + MA, ad hoc | Nothing obvious yet |
| Growing | 40–60 | Split across 3–4 roles | Interaction thresholds slipping |
| Strained | 75–100 | Everyone and no one | Billing gaps, missed alerts |
| Broken | 100+ | Escalated to clinicians | Revenue leakage, compliance risk |
The loop that needs to run monthly device check, threshold review, patient contact, EHR note, and CPT submission, is being executed by four different people with four different primary responsibilities. Each step gets done eventually. The handoffs are where the program bleeds. Learn more about appointment setting assistant for hire.
The Threshold Where It Becomes Undeniable
For most practices, the inflection point hits between 75 and 150 enrolled RPM patients. Below that, the fragmented workflow produces uneven results but doesn't fully collapse. Above it, something breaks.
What the breakdown looks like:
- Clinicians get pulled back into coordination tasks they were supposed to delegate
- Billing inconsistencies accumulate across multiple monthly cycles
- Revenue targets get missed by 30–40% with no clear explanation
What usually triggers the realization:
- A billing audit or revenue cycle review surfaces months of incomplete or missing RPM claims
- The practice isn't just looking at a process problem, it's looking at a structural one that's been compounding quietly for 6–12 months
That's the moment RPM virtual assistant services move from "nice to have" to operationally necessary.
What RPM Virtual Assistants Actually Do
RPM virtual assistant services are purpose-built for the monitoring workflow, not borrowed from a general admin role. That specificity is what makes them effective.
What sets them apart from general VAs:
- Trained specifically on RPM workflows, EHR documentation standards, and CPT billing requirements
- Own the full monthly cycle, not just individual tasks
- Operate proactively, not reactively
Core responsibilities:
Device Data Review and Alert Management
- Monitors incoming readings against established thresholds
- Flags out-of-range data for clinical review without waiting for a clinician to notice
- Documents alerts and initiates patient outreach per protocol
Patient Outreach and Adherence Support
- Conducts the monthly interactive communication required for CPT 99457 billing
- Troubleshoots device issues and reinforces usage habits
- Documents every interaction with the specificity billing requires
EHR Documentation and CPT Billing Support
- Tracks time thresholds for 99453, 99454, and 99457 compliance
- Documents patient encounters accurately and consistently
- Supports the billing team with clean coding inputs to reduce denials
| Task | General VA | RPM Virtual Assistant |
|---|---|---|
| Device alert monitoring | ✗ | ✓ |
| Patient outreach for 99457 | ✗ | ✓ |
| EHR documentation | Limited | RPM-specific |
| CPT billing support | ✗ | ✓ |
| Full monthly cycle ownership | ✗ | ✓ |
How RPM Virtual Assistants Fit Into Existing Practice Structure
An RPM virtual assistant doesn't replace clinical staff. They handle the coordination layer that clinical staff shouldn't be managing in the first place.
Wing's healthcare virtual assistants have delivered measurable results in clinical settings. At Provida Family Medicine and Bryant West Psychology, dedicated Wing VAs produced consistent, measurable outcomes by taking over the coordination layer:
- 35% reduction in billing errors
- 40% improvement in patient satisfaction
- 30% fewer scheduling errors
- 25+ hours per week saved on clinical admin
- 50% fewer emails and manual follow-ups
The pattern is consistent across practice types: when a dedicated role owns the administrative and coordination workflow, clinical staff stop absorbing tasks they weren't hired to do, and the operation runs cleaner.
Frequently Asked Questions
Do RPM virtual assistants have access to clinical decision-making?
No. RPM VAs handle coordination, documentation, and patient outreach, not clinical judgment. When a device reading requires a clinical response, the VA flags it for the appropriate provider. The care decision stays with the clinician; the workflow management stays with the VA. Wing's Remote Patient Monitoring VA and Patient Care Coordinator VA are trained specifically for this boundary — supporting the workflow without crossing into clinical territory.
How do RPM virtual assistant services handle HIPAA compliance?
Reputable RPM VA services operate under Business Associate Agreements (BAAs) and follow HIPAA-compliant communication and data handling protocols. Wing's HIPAA-Compliant Virtual Assistants are trained to handle protected health information correctly across all touchpoints, scheduling, documentation, billing support, and patient outreach. Confirm BAA terms during onboarding before deploying any VA into your RPM workflow.
Can an RPM virtual assistant handle billing support alongside monitoring tasks?
Yes — and that combination is where most of the revenue recovery happens. Wing's Medical Billing Specialist, Coding Specialist, and Prior Authorization Specialist can work alongside your RPM VA to ensure CPT codes 99453, 99454, and 99457 are documented accurately and submitted cleanly, reducing denials and capturing revenue that fragmented workflows routinely miss.
The Shift That Makes RPM Programs Work at Scale
RPM program underperformance is rarely a technology problem. The devices work. The clinical rationale is solid. The reimbursement model is viable.
What fails is the operational structure, specifically, the assumption that an existing team can absorb a continuous, time-sensitive monitoring workflow on top of their current responsibilities. That assumption holds at low volume. It breaks at scale.
The structural correction is straightforward: assign dedicated ownership to the workflow. RPM virtual assistant services are built for exactly that role. They don't add complexity. They remove the fragmentation that's already there.
Practices that make this shift stop treating RPM as a side process and start running it as the structured program it was designed to be.
Ready to close the workflow gap in your RPM program? Book a free demo with Wing and see how a dedicated RPM virtual assistant fits your current setup.

Dianne Florendo is a content writer who creates engaging SEO content about virtual assistants, outsourcing, and business productivity.



