





TL;DR
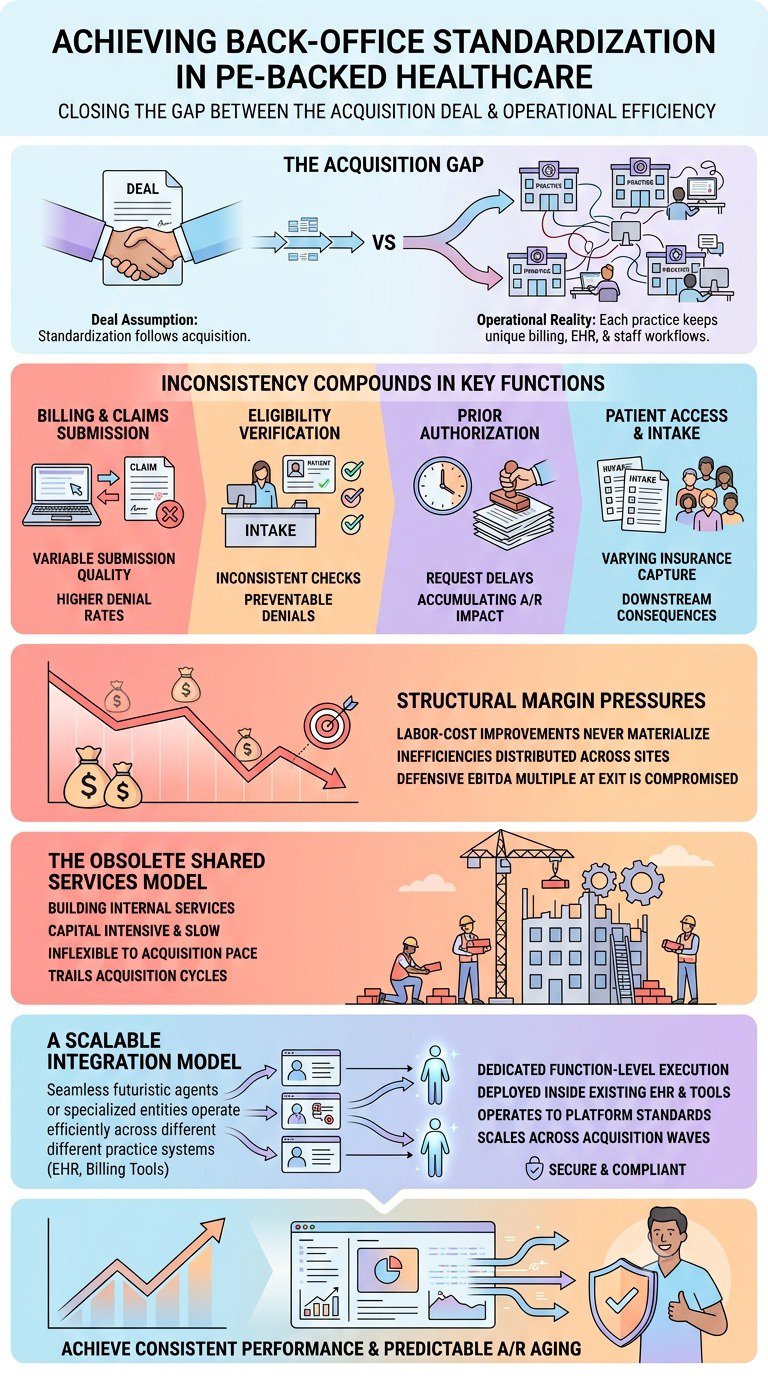
Most PE healthcare deals assume back-office standardization will follow the acquisition. In practice, each acquired practice runs its own billing workflows, EHR configuration, and staff habits, none of which match the platform standard. Without dedicated function-level ownership during the transition, platforms carry inconsistent back-office performance indefinitely, and the labor-cost improvement the margin thesis depends on never materializes.
The Integration Assumption Every Deal Makes
The LOI is signed. The deal closes. Integration is "underway." The 100-day plan has a slide deck. And somewhere in the financial model, back-office standardization is assumed to happen within 12 months, because the math doesn't work if it doesn't.
This is how most PE-backed healthcare BPO services acquisitions begin. It's also where many of them start losing ground before anyone notices.
The assumption isn't unreasonable on paper. You're buying a practice or a group of practices. You have an operating platform. You have systems, workflows, and billing protocols that work. The acquired entity plugs in. Performance normalizes. Margins improve.
What the model doesn't account for is the actual labor involved in getting a practice from where it is to where it needs to be, at the function level, not the IT level.
What Actually Happens After Close
The IT migration gets managed. Credentialing gets transferred. The EMR gets stood up under the platform's instance. A few operational leads hold kick-off calls. And then, the practice keeps running the way it always has, because nobody owns the transition at the task level.
Billing staff still follow the workflows they were trained on at the old organization. Eligibility checks still happen the same way, or don't happen consistently at all. Prior authorization requests still go through whoever submits them by habit. Patient access, scheduling, intake, insurance capture vary by location, by staff, and by whoever showed up that day.
This isn't a failure of intent. It's a structural gap. Integration plans assign ownership at the system level (IT migration, policy rollout, reporting) but rarely at the function level (who is actually working the billing queue at Site 7 the way the platform needs it worked). Those are different things, and conflating them is how performance variability becomes permanent.
The industry is large enough that this pattern is playing out at scale. Private equity has acquired an estimated 44,000 physician practices since 2019, and PE now accounts for roughly 6.5% of physician practices, up from 4.5% in 2022. In dentistry, DSO affiliation is projected to rise from approximately 23% to 39% of dental offices by 2026. Each of those acquisitions carries the same integration assumption, and most face the same execution gap.
Where the Gap Shows Up
The functions where inconsistency compounds most visibly are also the functions that drive the margin thesis.
Billing and claims submission
Each acquired practice has its own patterns: how claims are coded, how modifiers are applied, and how secondary billing is handled. Without standardized workflows owned by someone accountable for output at each site, submission quality varies, and denial rates follow. The industry-wide initial claim denial rate hit 11.81% in 2024. A platform that hasn't standardized submission workflows across sites will see significant spread around that number, some locations performing better, others materially worse, with no clear mechanism to close the gap.
Eligibility verification
Eligibility is the front end of the revenue cycle. When it isn't verified consistently, or is verified too far in advance and not re-checked at the point of service, practices absorb downstream denials that were preventable at intake. This is a workflow ownership problem. Someone has to be checking eligibility the right way, at the right time, every time, at every site. A Medical Insurance Verification Specialist doing this function correctly at every location is the difference between a systemic process and a best-effort approximation.
Prior authorization
Prior auth is the highest-friction point in most specialty and procedural environments. It requires coordination between the clinical team, the payer, and the patient, often across multiple touchpoints and timelines. Without dedicated ownership, prior auth requests fall behind, procedures get delayed or denied, and the AR impact accumulates. A Denials Management Specialist working prior authorization systematically across locations is not optional if the platform intends to reduce its denial rate.
Patient access and intake
Insurance capture at intake, what information is collected, how it's verified, what triggers follow-up directly determine how many claims are clean at submission. When this varies by location and by staff member, the downstream revenue cycle carries the consequences. A Healthcare CSR owning intake workflows at each site closes the gap at the source.
Each of these functions requires dedicated ownership. Not a policy document. Not a training session at go-live. Ongoing, accountable execution that matches the platform's standard requirements.
The Margin Impact Is Structural
The reason this matters to the deal isn't operational; it's financial.
The margin thesis in most PE healthcare BPO services depends on labor-cost ratio improvement over time. Standardized workflows mean a leaner headcount relative to revenue. Standardized billing means consistent collections performance. Consistent performance across sites means the EBITDA multiple is defensible at exit.
When back-office functions aren't standardized, the labor-cost trajectory doesn't improve on its own. Sites that deny at 14% instead of 11% are paying staff to work claims that shouldn't have been denied. With inconsistent eligibility verification are absorbing write-offs that don't appear in the operating review until the quarter closes. Sites with underfunded prior authorization functions are generating delays that suppress revenue without appearing directly in any single line item.
The aggregate effect is that the platform's back-office never reaches the performance baseline the model assumed, and the labor-cost ratio doesn't improve because the inefficiency isn't concentrated; it's distributed across 8 or 12 or 20 sites, none of which looks catastrophic on its own.
PwC's 2024 data found that 40% of executives plan a major operating-model reorganization, a figure that reflects, in part, how structural these margin pressures have become.Healthcare BPO services aren't restructuring because they misread the market. They're restructuring because the back-office assumptions built into their models didn't survive contact with multi-site integration reality.
The Headcount Trap
The standard response to this problem is to build internal shared services. Centralize billing. Hire a team of eligibility specialists. Build a prior authorization function. Create a credentialing center of excellence.
This is the right conceptual direction and the wrong execution model for most PE-backed platforms at their current scale.
Building internal shared services requires capital, time, and a stable organizational structure. Capital is committed to the next acquisition, not to a back-office buildout. Time runs at acquisition pace, not implementation pace. And the organizational structure is rarely stable, a Credentialing Coordinator hired for Site A doesn't automatically scale to cover Sites B through E when the next deal closes six months later.
The headcount model also doesn't flex in the right direction. If the platform adds three locations in a quarter and loses one, the internal shared services team is either over- or under-resourced, and there's no fast mechanism to right-size it. Hiring and onboarding new back-office staff at platform scale is a multi-month cycle, which means the new acquisition runs its own back-office way longer than the integration plan assumed.
The result is that shared services builds often trail the acquisition pace by several cycles, which means the standardization benefit arrives late, if it arrives at all, before the next wave of acquisitions makes the problem more complex again.
What a Scalable Integration Model Actually Requires
The functions that undermine margin performance in multi-site PE healthcare BPO services- billing, eligibility, prior auth, patient access, credentialing- share a common requirement: dedicated ownership that operates consistently across locations without requiring a full-time hire at every site.
That's the model Wing provides. Wing Medical Billing Specialists and back-office assistants are AI-trained and deployed inside the platform's existing EHR and billing tools. They operate to the platform's workflow standards, not to whatever the acquired practice did before. And they scale across the acquisition wave, adding function-level capacity at each new site without triggering a separate hiring and onboarding cycle.
Wing is ISO 27001 compliant and SOC 2 certified, which matters in a regulated environment where the vendor is working inside your EHR and handling patient billing data.
The practical difference is that the platform gets function-level ownership at each site without the capital commitment and organizational complexity of building internal shared services. The back-office performs to standard from the start of integration, not after a 12-month ramp that assumes workforce stability, which the acquisition environment rarely provides.
This is what consistent denial rates and predictable A/R aging across locations actually require. Not a better policy deck. Not another integration kick-off call. Dedicated back-office execution, owned at the function level, that matches the platform standard regardless of what the acquired practice did before.
The Integration Gap Is Addressable: But Not With the Current Model
PE healthcare BPO services aren't failing on back-office standardization because the people involved aren't capable. They're failing because the model assumes standardization will happen as a byproduct of systems migration and policy rollout, when what actually produces it is function-level ownership that someone is accountable for delivering, consistently, across every site.
The healthcare BPO model that closes this gap isn't about outsourcing. It's about putting the right ownership structure at the function level, at platform scale, without requiring the capital and organizational build that internal shared services demand.
Until platforms close this gap, the margin thesis stays aspirational. The back-office performance the model assumed is achievable; it just requires a different approach to who owns it and how.
See how Wing supports back-office standardization across multi-site platforms → Book a Demo

Dianne Florendo is a content writer who creates engaging SEO content about virtual assistants, outsourcing, and business productivity.



